3d3bb467-e9ed-4611-87cd-e46c025ac32b.webp?sfvrsn=a1b7a841_3 "9781284229417-1-(1)")
 This is the fourth post in a five-part series where we'll give you a look inside this important new COVID-19 resource. In case you missed it, we recommend viewing the series in order, starting with Part One.
This is the fourth post in a five-part series where we'll give you a look inside this important new COVID-19 resource. In case you missed it, we recommend viewing the series in order, starting with Part One.
As an EMS provider, staying safe through the evolving COVID-19 situation involves distinct challenges. That's why the Public Safety Group, in partnership with the American Academy of Orthopaedic Surgeons, is pleased to introduce Evolution of EMS: COVID-19 Guidance for EMS Providers. This unique resource offers strategies and insights designed specifically for you.
This excerpt looks at treatment strategies and some promising studies for COVID-19.
Evolution of EMS: COVID-19 Guidance for EMS Providers describes the SARS-CoV-2 virus and disease, prevention tactics, vaccine development, treatment, and public health implications, particularly as they affect providers working in the field. It’s not designed to supply everything you need to know about COVID-19, but rather to brief you on key issues and considerations. COVID-19 Guidance for EMS Providers also offers references for learning more and staying up to date. The goal: empowering you to protect yourself, your co-workers, and those you serve more efficiently and effectively.
There are three easy ways to access COVID-19 Guidance for EMS Providers:
- Stay Tuned to the Public Safety Group Blog:
New excerpts will be rolled out on our Public Safety Group blog on a biweekly basis, free of charge (Part One is available here, Part Two is available here, Part Three is available here, Part Four is available below, and Part Five is available here)
- Sign Up to Receive a Free, Complete Copy of the Resource:
Visit http://go.psglearning.com/COVIDGuidanceNow to request your free copy today. We'll email you a PDF to download as soon as the complete resource is available later this Fall:
I Want to Request My Free PDF:
COVID-19 Guidance for EMS Providers
- Purchase Physical Copies of the Resource on our Website:
Visit http://go.psglearning.com/COVIDGuidance to pre-order your physical copy which will be available later this Fall
Questions? Please contact your dedicated Public Safety Specialist today.
Part Four: Treatment Strategies
As of October of 2020, definitive treatments for COVID-19 are in development. Clinical trials of antivirals, channel blockers, and other approaches are under way, and outcome evidence from the studies is being analyzed and peer-reviewed. Some promising studies include the following:
- SIMPLE, CARAVAN, and ACTT-1, -2, and -3. Based in the United States, these multicenter randomized controlled trials (RCTs) are studying remdesivir in different settings.
- RECOVERY. This study, based in the United Kingdom (Oxford), is exploring use of dexamethasone/azithromycin/tocilizumab/convalescent plasma.
- REMAP-CAP. This international collaborative effort is studying multiple treatments for all community-acquired pneumonia.
- CATALYST. Based in the United Kingdom (Birmingham), this study is investigating multiple medications to decrease intensive care unit (ICU) admissions.
- REALIST. This study, based in Ireland (Belfast), is investigating umbilical stem cell therapy.
- I-SPY. Based in Japan, this study is examining several repurposed medications, including a bradykinin antagonist.
- DART. This study, based in the United States (Johns Hopkins University), is investigating the effectiveness of decitabine.
- ACTIV series. Based in the United States, these multicenter RCTs are studying heparin and anticoagulation therapies.
Jumping to premature conclusions about these treatments can ultimately result in delays and even poor outcomes. Many pharmaceutical treatments in the trial phase have significant side effects to patients. Properly addressing all issues and developing widely effective treatments can take months or years, even on a fast-tracked schedule.
For EMS providers, it is important to align with approved treatment protocols while understanding limitations in the medical community. Current treatment plans for people with mild symptoms of COVID-19 include self-isolation at home, rest, and fluid intake. Treatments for those with severe symptoms requiring hospitalization focus on supporting ventilation and circulation by providing fluids and oxygen.
EMS protocols often involve specific devices and PPE considerations when managing a patient’s oxygenation and fluid level requirements. Critical COVID-19 patients may need aggressive hemodynamic and ventilatory support, including invasive airways, positive pressure ventilation (PPV) devices, and pharmacologic blood pressure support. For nonintubated patients, limited studies suggest that placing the patient in a prone position (proning) can help improve respiratory and final outcomes, though more research is needed (Coppo et al. 2020). There is no evidence as of yet of any benefit in placing patients in a prone position for short periods of time, such as the time periods associated with typical EMS transports. The risks of limiting access to the patient's airway and limiting the ability to monitor the patient may outweigh the benefit of prone positioning in most EMS scenarios.
Diagnosis
Pneumonia is a dangerous lung infection that can, as in the case of COVID-19, be deadly. Those at highest risk are very young children and older adults. Pneumonias are classified as viral, bacterial, or fungal. Viral and bacterial pneumonias are more common than fungal and can spread from person to person through the inhalation of droplets and aerosols. All three types can also exist concurrently.
A systematic review in 2020 of patient care records revealed that between 10% and 29% of traditional pneumonia patients will have both bacterial and viral infections simultaneously (Heneghan, Pluddemann, and Mathani 2020). A 2016 systematic review and meta-analysis of 31 published pneumonia studies included more than 10,000 patients and drew similar conclusions, showing that approximately 25% of patients had both viral and bacterial infections (Burk et al. 2016). Despite this trend, early cases of this novel CAP (COVID-19) did not frequently demonstrate coexisting bacterial pneumonia. Distinguishing the origin was crucial in providing the right care to each patient at the right time (Figure 4-1).
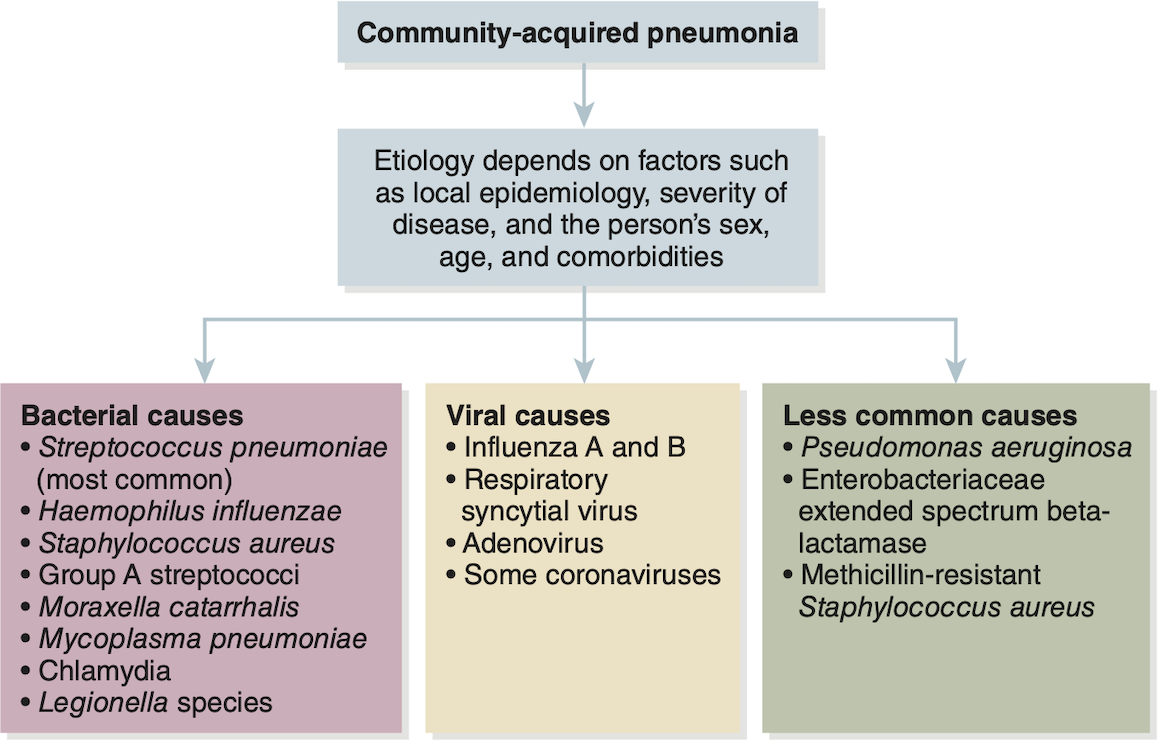
Figure 4-1: Distinguishing among community-acquired pneumonias.
Used with permission from Carl Heneghan, Oxford COVID-19 Evidence Service Team, Centre for Evidence-Based Medicine, Nuffield Department of Primary Care Health Sciences, University of Oxford. 2020.
The most common origins of pneumonia often can be ruled in or out based on clinical presentation and diagnostic testing. Rapid flu swabs are usually performed first and return results within 5 to 15 minutes. Several different microbes can cause bacterial pneumonia, which can be cultured through sputum samples. Sputum tests take longer to provide results but are still extremely important.
Bacterial pneumonias are one of the most common triggers for sepsis, which can progress quickly to septic shock. The Surviving Sepsis Campaign, from the Society of Critical Care, describes a bundle of care called early goal-directed therapy for these patients. This bundle includes early fluid, early antibiotics, and vasopressors when indicated.
When differentiating between viral and bacterial pneumonias, it is helpful to compare and contrast clinical symptoms and diagnostic tests (Table 4-1). Disease progression rates often differ between COVID-19 patients and patients with more traditional bacterial pneumonia. The presence of discolored or foul-smelling sputum is more often seen in bacterial pneumonia. Though fever can be present in both, it more often results from bacterial pneumonia.
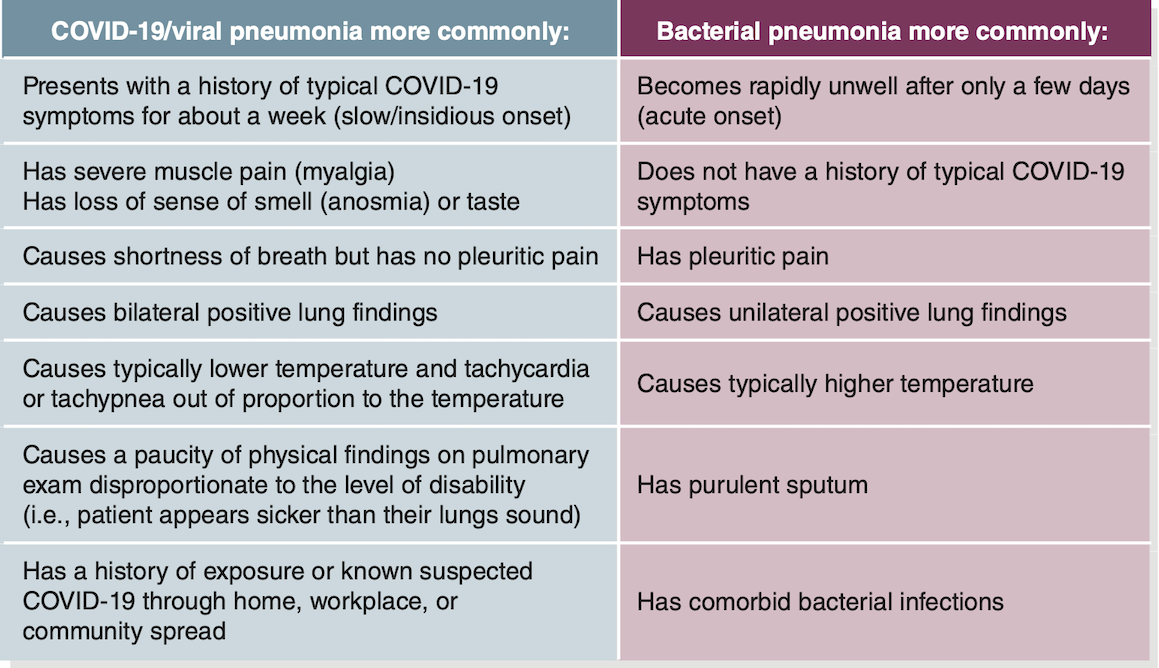
Table 4-1: Differentiating COVID-19 From Bacterial Pneumonia
Used with permission from Carl Heneghan, Oxford COVID-19 Evidence Service Team, Centre for Evidence-Based Medicine, Nuffield Department of Primary Care Health Sciences, University of Oxford. 2020.
Treatment: An Evolving Set of Strategies
Initially, sepsis was of central concern for patients critically ill with COVID-19 because of high mortality and the association with pneumonia. However, respiratory failure and multiple organ failure often occurred in the absence of bacterial pneumonia. Today, the central concerns in treating COVID-19 patients include respiratory failure, so-called cytokine storm, and certain types of coagulopathy, including disseminated intravascular coagulation.
Respiratory Failure
The most common inflammatory markers of COVID-19 are tachycardia and tachypnea. In the early months of the COVID-19 pandemic, early respiratory failure and ARDS appeared to develop in patients. Radiographic studies of COVID-19 patients often revealed bilateral opacities (Figure 4-2). Computed tomography (CT) scans with bilateral ground-glass opacities became a hallmark of this disease. This radiographic pattern is a marker for fluid filling the lungs. When fluid invades the alveoli, exchange of oxygen and carbon dioxide is inhibited.
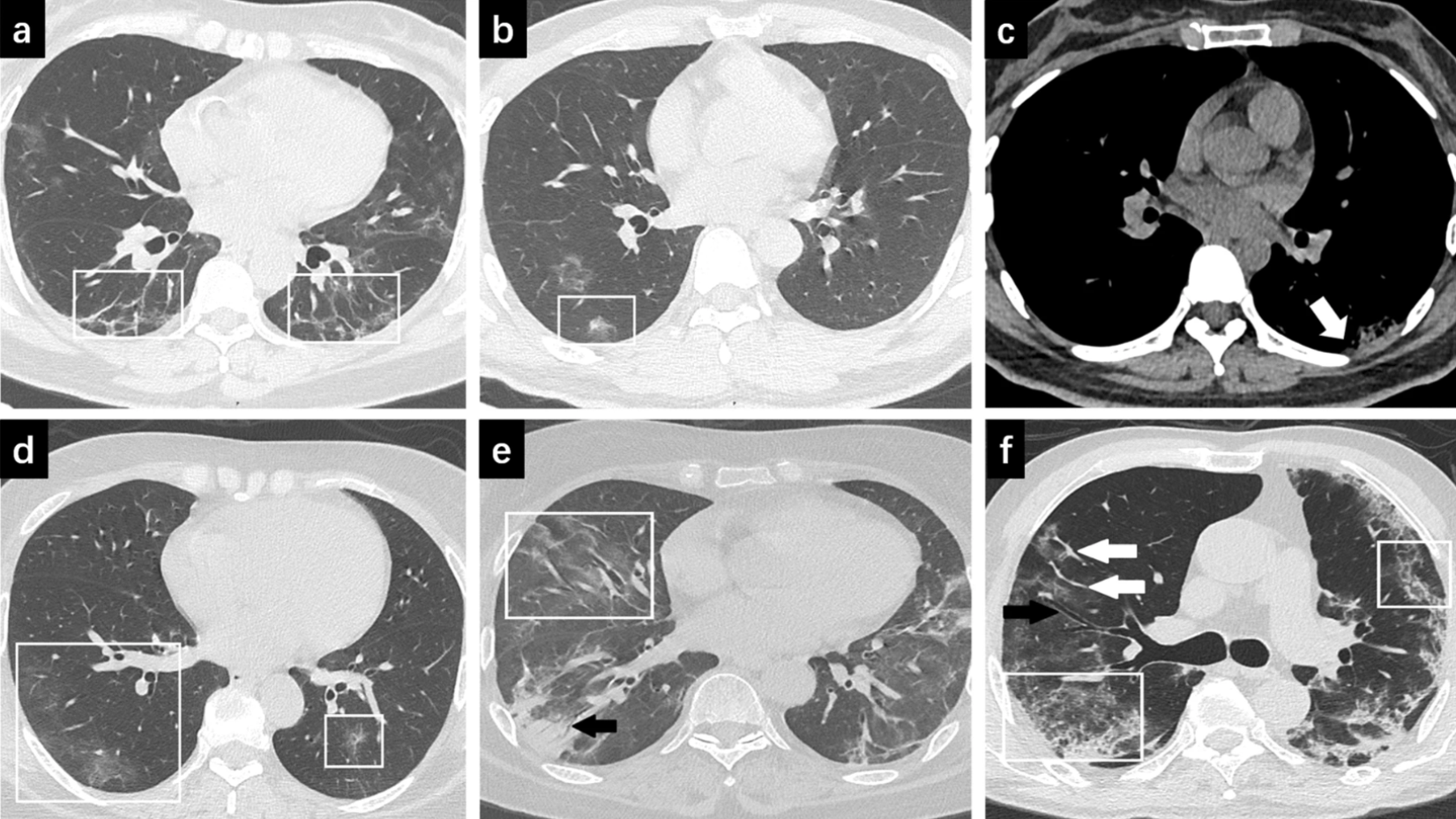
Figure 4-2: Ground glass opacities in COVID-19 patient scans.
Reproduced from Fu Z, Tang N, Chen Y, et al. 2020. “CT Features of COVID-19 Patients With Two Consecutive Negative RT-PCR Tests After Treatment." Sci Rep 2020;10:11548.
Figure 4-2 shows the following:
-
-
- Scan A. 56-year-old woman with moderate COVID-19. CT image shows pulmonary fibrosis in both lungs (see white boxes).
- Scan B. 37-year-old man with moderate COVID-19. CT image shows mixed ground glass opacity (see white box).
- Scan C. 32-year-old woman with moderate COVID-19. CT image shows thickening with pleural adhesion (see white arrow).
- Scan D. 50-year-old woman with severe COVID-19. CT image shows ground glass opacities in both lungs (see white boxes).
- Scan E. 59-year-old woman with severe COVID-19. CT image shows ground glass opacities (see white box) and consolidation with air bronchogram in the right lung (see black arrow).
- Scan F. 65-year-old man with severe COVID-19. CT image shows bronchial wall thickening and abnormal widening of the airways (see black arrow). Vascular enlargement is also apparent (see white arrows). The white outlines also show pulmonary tissue thickening in both lungs.
- Scan A. 56-year-old woman with moderate COVID-19. CT image shows pulmonary fibrosis in both lungs (see white boxes).
-
Initial respiratory management targets maintaining an adequate level of oxygen saturation (92% to 96%). Many early COVID-19 observational reports and studies identified patients who presented with hypoxia disproportionate to their dyspnea. Subsequently, the phrase “happy hypoxia” started to appear in the differential diagnosis for COVID-19. This paradoxical concept is not new. It first appeared in pulmonary/ARDS literature to describe patients who did not appear short of breath but whose oxygen saturation levels measured low (or extremely low). High-flow nasal cannulas and noninvasive positive pressure ventilation have become first-line treatments for these symptoms.
High-flow nasal cannulas are not just regular cannulas turned up high. These specialized nasal cannula systems, using devices such as the Fisher & Paykel Optiflow or Vapotherm Precision Flow, can deliver 50 to 60 liters per minute of warm humidified oxygen (Figure 4-3).

Figure 4-3: A high-flow nasal cannula.
© Jones & Bartlett Learning.
The warmth and humidity help decrease the inflammation that can occur because of traditional nasal cannula or nonrebreathing systems that are both cold and dry. This type of device also helps maintain the ciliary function in the cells that line the respiratory tract. This type of respiratory assistance does not heal or cure COVID-19; rather, it supports the body long enough to hopefully allow it to recover.
As the respiratory symptoms increase in severity, the treatments and interventions also become increasingly aggressive. Proning is one bridging strategy that can help prevent the need for invasive ventilation. When the alveoli begin to collapse or fill with fluid, the patient may feel increasingly short of breath. By positioning the patient in the prone position, the posterior rib cage can expand with greater volume. Several observational studies performed in Italy have shown that proning can increase alveolar recruitment and improve oxygenation and ventilation. This treatment has been evolving for several years in the ICU as one solution to patients with refractory ARDS. In the studies, the patient usually was intubated, and large equipment was required for the procedure every few hours. In the COVID-19 patient, proning is sometimes helpful when the patient is still conscious and able to self-prone. However, the experiences of some clinicians suggest that proning can improve outcomes for severe COVID-19 patients regardless of the oxygen delivery method, invasive or noninvasive (Caputo, Strayer, and Levitan 2020).
Proning can be combined with noninvasive ventilation. Continuous positive airway pressure (CPAP) has been a point of uncertainty in COVID-19 protocols since the beginning of the outbreak. Initially, many medical directors and administrators were advising departments to limit the use of CPAP due to the aerosolizing nature of the device. As the disease pathology becomes better understood, and the filter devices become more widely available, CPAP has seen a return to many treatment protocols. CPAP can be combined with proning to help prevent further respiratory decline and the need for invasive ventilation.
Patients in whom ARDS or respiratory failure develops will often require invasive ventilation by endotracheal intubation. These patients require increasing positive end-expiratory pressure (PEEP) to keep the alveoli open and to maintain adequate oxygenation. According to an early 2020 study, ARDS “is the most common indication for transferring patients with COVID-19 to the ICU and the major cause of death in this patient population” (Salehi et al. 2020). The study also found that any clinical improvement usually occurs after week 2.
Up to this point, because pneumonia in the ICU had been primarily bacterial in nature, many critical care physicians and staff used guidance from the studies generated from the Society of Critical Care Medicine and the Surviving Sepsis Campaign. These two organizations created a joint recommendation for COVID-19 ICU admissions and treatment pathways (Table 4-2).
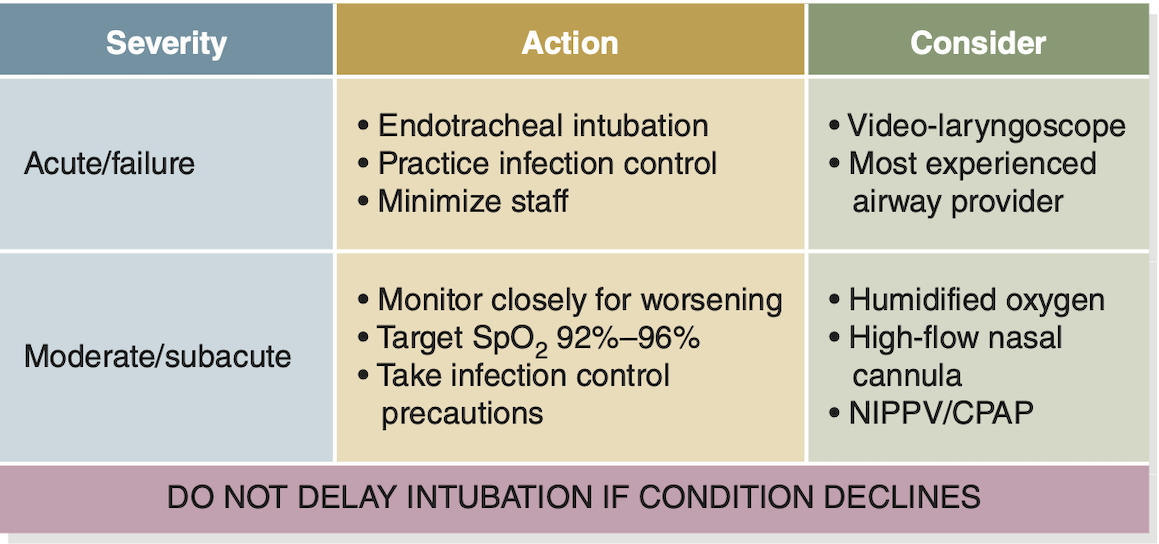
Table 4-2: Recommendations for Managing COVID-19 With Hypoxia
Based on resources from the Society of Critical Care Medicine and Surviving Sepsis Campaign.
*Abbreviations: CPAP, continuous positive airway pressure; NIPPV, Noninvasive positive-pressure ventilation; SPO2, oxygen saturation
Cytokine Storm
One of the contributors to ARDS development is the downstream effect of the inflammatory pathway. Interstitial and pulmonary tissues are damaged from a massive release of cytokines, which are small signal proteins that are released by cells during the inflammatory and immune cascade.
These cellular cascades operate much like the valves in an air/oxygen tank-filling cascade. When the SARS-CoV-2 invades, it takes over the signaling system and essentially opens all the valves at once, flooding the surrounding tissue with the cytokines. This process is referred to as a cytokine storm. In a patient with COVID-19, “the inflammatory cytokine storm is closely related to the development and progression of ARDS” (Ye et al. 2020). Historically, ARDS is an extremely critical state that is often associated with poor patient outcomes. In COVID-19 patients, researchers found “the serum levels of cytokines to be significantly increased in patients with ARDS,” with the degree of increase being “positively correlated with mortality rate” (Ye et al. 2020).
Early case reviews suggested that the bigger the cytokine storm, the higher the mortality rate. Larger studies are starting to show a less dramatic cytokine response in patients with COVID-19 versus patients with ARDS (Cummings et al. 2020). This finding has resulted in a downshift in some treatments targeting the cytokine cascade. However, there are still some significant overlaps in the presentation and treatments for these two pathologies, so the concept of cytokine storm in COVID-19 has not yet been entirely abandoned.
Related Coagulopathies
In addition to the pathologies discussed thus far, at least two pathologic coagulation processes appear to occur in critically ill COVID-19 patients. As one study found, “In the microcirculation of the lung and potentially other organs, there is local direct vascular and endothelial injury-producing microvascular clot formation” (Iba et al. 2020). In the systemic circulation, there is hypercoagulability and hyperactivation of fibrinogen, creating the potential for thrombosis and significant downstream effects, such as pulmonary embolism, stroke, or heart attack. A high index of suspicion for COVID-19 should be maintained in all patients presenting with conditions involving clot formation or embolization.
Although disseminated intravascular coagulation is a hallmark of late sepsis, COVID-19 coagulopathy is markedly different. Providers draw routine sequential coagulation studies, including platelet counts, D-dimer levels, prothrombin time, and partial thromboplastin time. These tests allow clinicians to determine if the clotting cascade has been affected by COVID-19 and whether the patient needs anticoagulation therapy. In severe cases, thrombectomy is a part of the COVID-19 treatment strategy.
Kidney Problems
In addition to the respiratory pathology and coagulopathy, a high percentage of COVID-19 patients are presenting with signs and symptoms of kidney problems. Pei et al. (2020) identified that “renal abnormalities occurred in the majority of patients with COVID-19 pneumonia.” ICU patients with COVID-19 very often present with this pathology. According to the same study, “Although proteinuria, hematuria, and acute kidney injury (AKI) often resolved within 3 weeks after the onset of symptoms, renal complications in COVID-19 were associated with higher mortality” (Pei et al. 2020). Microvascular injury and coagulopathy may be significant contributors to renal dysfunction.
For EMS providers, the downstream concerns of kidney problems include electrolyte derangements and hemodynamic fluctuations. The investigators in this study concluded the patients with acute kidney injury often demonstrated a worse course. It is possible that the microvascular injury and coagulopathy were major contributors to renal dysfunction.
Hospitalizations: Rates and Trends
As the COVID-19 situation evolves, reporting and analysis of hospitalization rates continue to evolve. On June 28, 2020, the CDC reported that the United States had more than 2.5 million cases of COVID-19, with 125,000 deaths. The overall cumulative hospitalization rate was 98.4 per 100,000 population, meaning approximately 0.1% of the country had been hospitalized for COVID-19. It is important to note that hospitalization numbers are usually delayed by approximately 2 weeks because they require COVID-NET data from hospitals.
Total hospitalizations have continued to rise in the United States. The highest rate of hospitalization remains among adults aged 65 years or older, followed by adults aged 50 to 64 years, then those aged 18 to 49 years (Figure 4-4). The total number of deaths has also risen. By October 13, 2020, the CDC reported that the United States had almost 7.8 million cases of COVID-19, with 214,446 deaths.
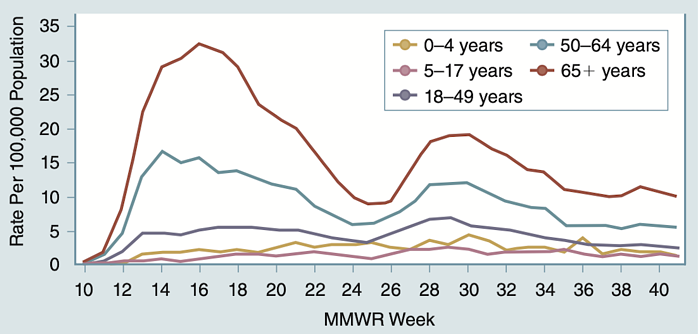
Figure 4-4: Hospitalization rates by age group.
From COVID-NET: COVID-19-Associated Hospitalization Surveillance Network, Centers for Disease Control and Prevention. Accessed October 19, 2020.
*Abbreviations: MMWR Week, Morbidity and Mortality Weekly Report
Drug Development: Highly Targeted and Fast-Tracked
The process of discovering, developing, and eventually manufacturing new medications has changed significantly in recent years. Classic pharmacology looked at the active ingredients of current treatments and tried to line them up with the target disease process. With advances in the use of the human genome, the process today is entirely different, with high throughput screenings against biologic targets.
In the case of SARS-CoV-2, the genome of the virus was mapped and shared in early 2020, enabling the process of drug discovery to be targeted at the different phases and steps in the disease cascade.
In one illness framework, developed by Dr. Salim Rezaie, an emergency medicine physician, the disease process is separated into three phases: viremic, pulmonary, and severe (Table 4-3).
- During the viremic phase, the viral load of the patient rises sharply, and pharmacology development is being targeted to mitigate the viral replication. Antiviral medications work to interrupt that process.
- If the disease progresses to the pulmonary phase, the inflammatory cascade begins to rise sharply. As discussed previously, a dangerous part of the disease process involves an exaggerated inflammatory response and the resulting ARDS and acute kidney injury. Medications focused on blunting the inflammatory response are most effective here. In July 2020, the RECOVERY trial published a set of recommendations regarding dexamethasone during this phase.
- The severe phase has high mortality rates. This phase requires aggressive anti-inflammatory and anticoagulation therapy.
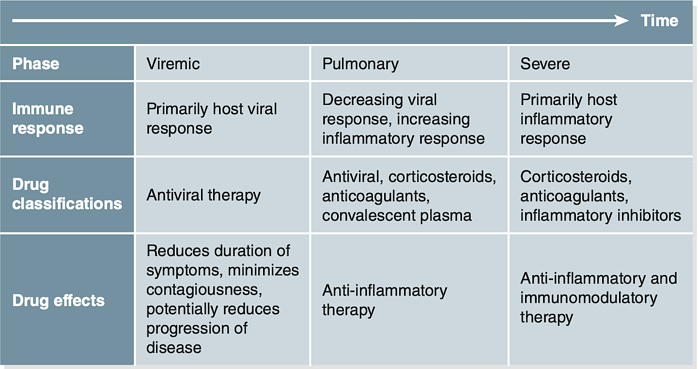
Table 4-3: Framework for COVID-19 Phases and Treatment Suggestions
Based on Rezaie, S: The RECOVERY Trial: Dexamethasone for COVID-19?
Trials and Approaches
Development of COVID-19 drugs and therapies continues on several fronts. The FDA created a special coronavirus treatment acceleration program (CTAP) in April 2020 to help get treatments to patients faster. In July, the CTAP dashboard counted more than 570 drugs in the developmental stage and at least 270 trials under review. By August 2020, CTAP displayed 590 drugs in development, 310 trials under review, and 5 drugs approved for emergency use. The August 31, 2020, emergency use authorization (EUA) covers convalescent plasma, remdesivir, and several other emerging therapies (Figure 4-5).
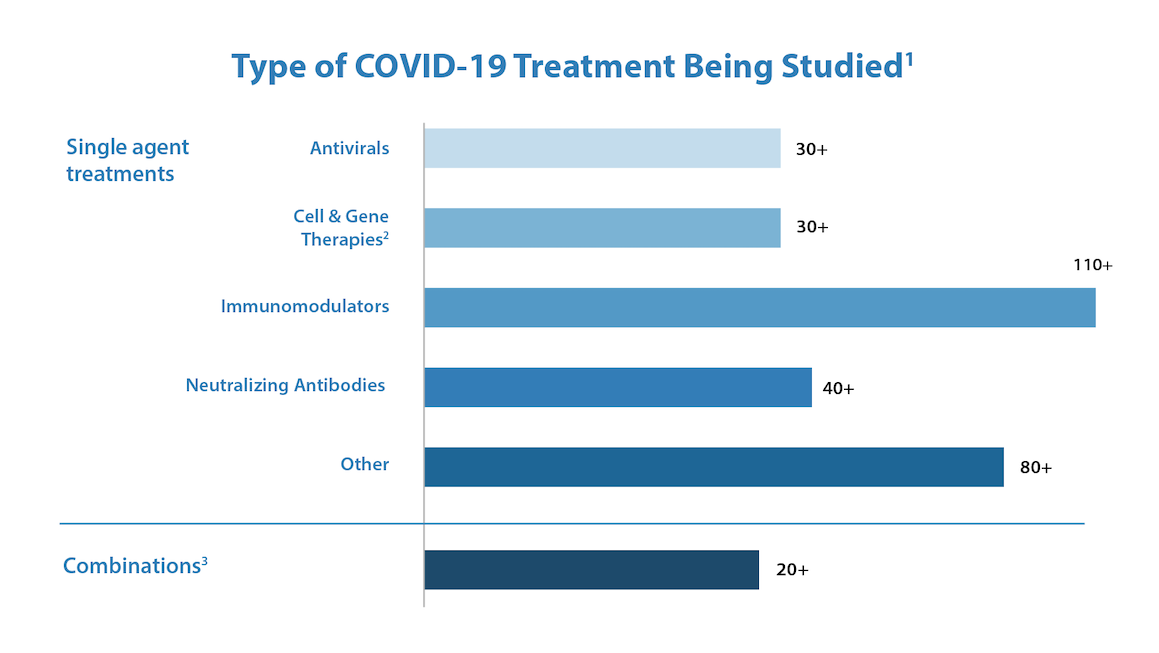
Figure 4-5: CTAP dashboard snapshot from August 2020.
US Food and Drug Administration. Coronavirus Treatment Acceleration Program (CTAP). Accessed October 15, 2020.
1. Corresponds to number of safe to proceed investigational new drugs (INDs); excludes INDs related to vaccines
2. For additional information, please see Cellular & Gene Therapy Products
3. Includes INDs with more than one product
About Emergency Use Authorization (EUA)
On February 4, 2020, the Secretary of HHS determined that SARS-CoV-2 had the potential to affect national security, and a public health emergency was declared. On March 27, HHS stated, “Circumstances exist justifying the authorization of emergency use of drugs and biological products during the COVID-19 pandemic.” This declaration allowed the FDA commissioner to issue EUA for some therapies to be used prior to completing a traditional cycle of trial and peer review when no other adequate therapies existed.
In May 2020, the National Health Service in the United Kingdom, in collaboration with the University of Birmingham, published a useful global overview of clinical trials (Figure 4-6). Although other significant studies have emerged since then, this overview helps illustrate the diversity of approaches across the pathologic cascade of events.
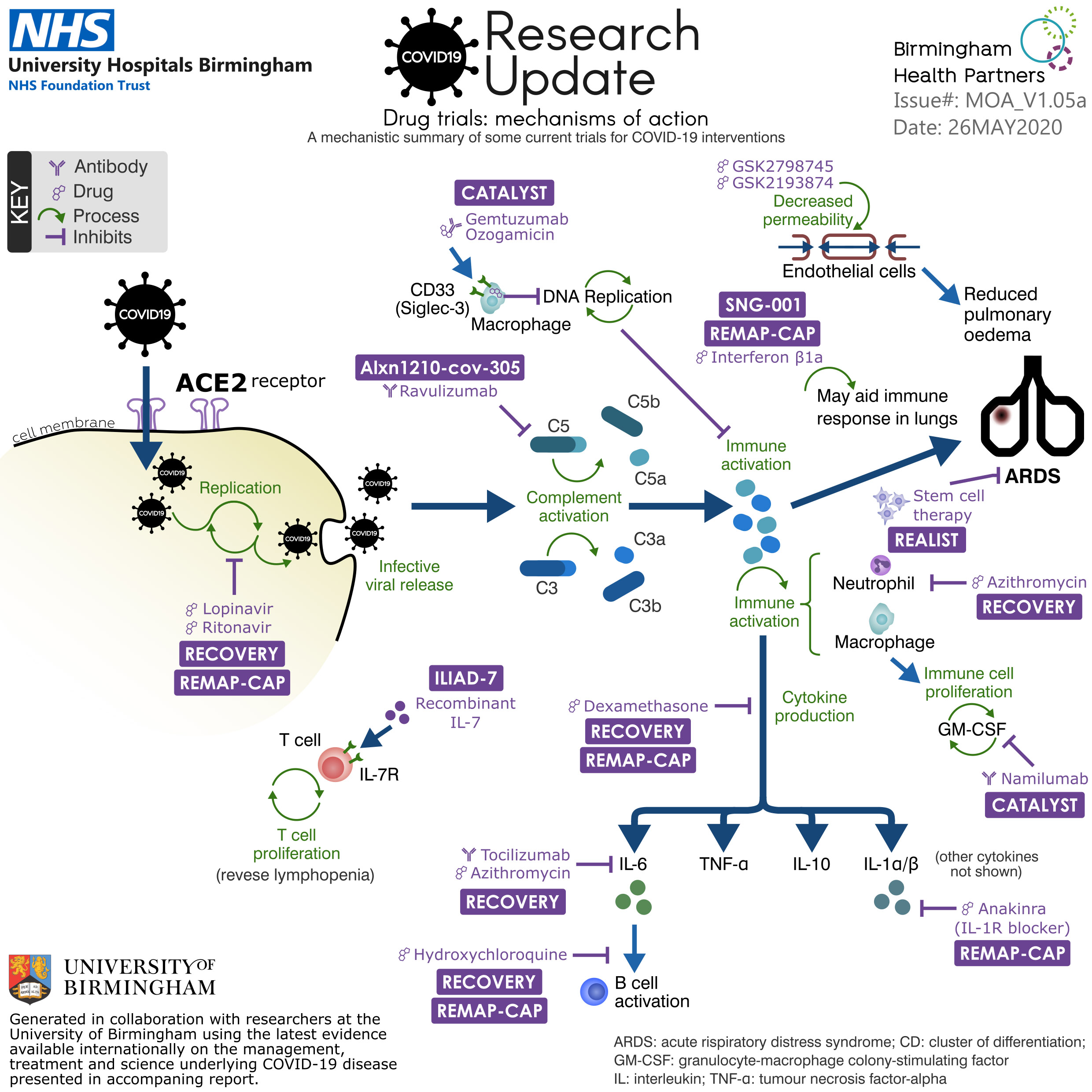
Figure 4-6: The worldwide approach to COVID-19 treatment clinical trials.
Used with permission of University of Birmingham.
With so many treatments and approaches in process, it may be useful to see the clinical picture in terms of treatment types:
- Antivirals, such as remdesivir, lopinavir, and ritonavir, are intended to work by blocking the initial replication of the RNA carried inside the coronavirus.
- Ravulizumab and gemtuzumab ozogamicin work by inhibiting the antibodies and complementary proteins needed in the next step of the cascade.
- GSK2798745 and GSK2193874 are channel blockers that decrease the permeability of the endothelial cells in the lungs, which helps reduce pulmonary edema. Similarly, interferon beta 1a and stem cell therapy are also being investigated to help protect against ARDS.
- Azithromycin is a macrolide antibiotic that degranulates, or inhibits the neutrophil response. It is also suggested that it may alter the packaging of the ACE-2 receptor and thus change the initial viral entry into the cell.
- Namilumab inhibits the immune cell proliferation downstream from the alveolar macrophages.
- Dexamethasone is showing promise in inhibiting the cytokine storm.
- Hydroxychloroquine inhibits the B cell activation and thus affects the inflammatory/immune cascade.
- Icatibant, a bradykinin B2 receptor antagonist, is intended to interrupt the endothelial hyperinflammatory reaction.
Another notable therapy is convalescent plasma. Patients who have recovered from COVID-19 retain some of the antibodies in high enough quantities that they can be beneficial to other patients (Figure 4-7). A plasma donation from a recovered COVID-19 patient can potentially help up to three additional patients, depending on how soon after the disease donation occurs. This treatment is currently allowable as an investigational treatment under the FDA’s EUA program.
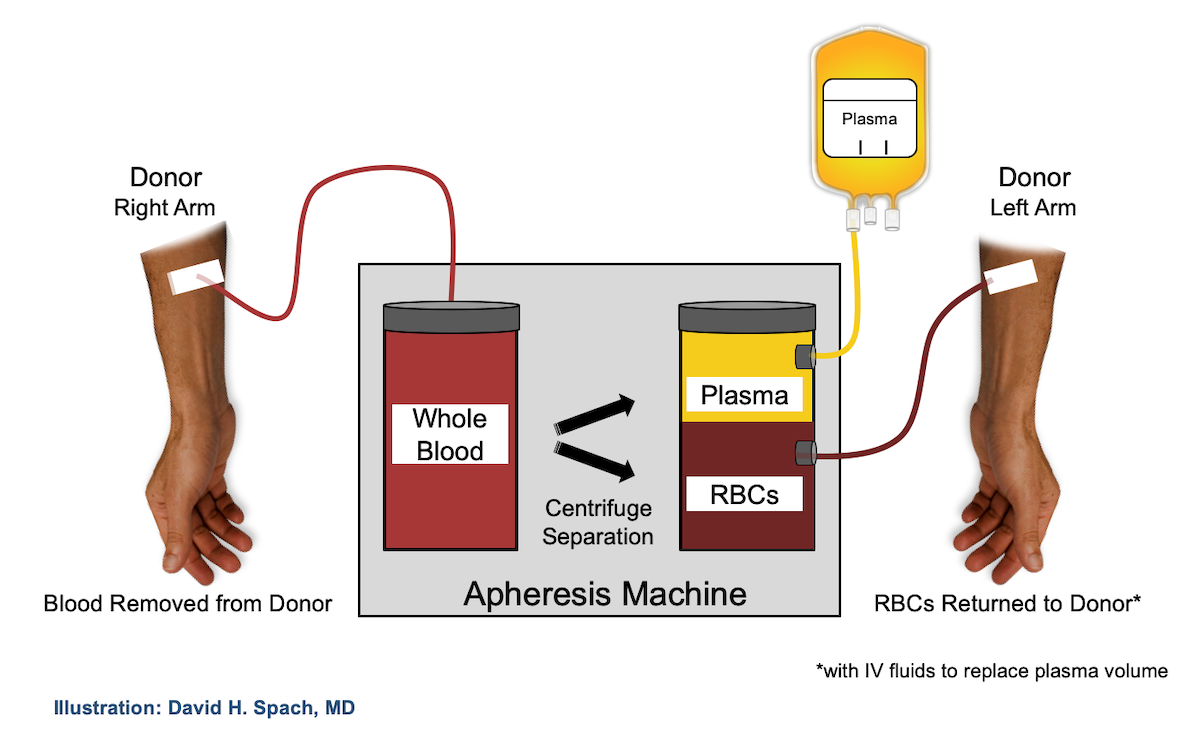
Figure 4-7: The convalescent plasma process.
David H. Spach, MD.
Although potentially promising, these treatments are relatively early in their accelerated trials. Researchers are carefully monitoring efficacy, side effects, interactions, and other issues as they advance toward effective treatments.
Considerations for EMS Providers
Most treatments and trials are designed for the in-hospital treatment of patients with COVID-19. Dexamethasone is the only trial medication that is currently available to some prehospital providers. Treatment protocols will be determined by the EMS agency. Oxygen administration combined with strategies such as CPAP can be extremely helpful in managing COVID-19 patients at the scene. Most services that provide CPAP are familiar with how to transport and filter the device safely.
Patient safety becomes a major concern when proning is considered during transport. Seat belts and harnesses are not usually designed for prone transport. Also, sudden deterioration would be extremely difficult to manage alone, in the back of a moving ambulance, for a patient being transported in the prone position. When considering the risks and benefits for transport procedures, exercise additional caution regarding prone patients and seek specific guidance from your medical director. The value of short-term proning in the EMS environment has not been clearly established in this or any other population of patients.
The acuity of COVID-19 symptoms remains quite variable, and the challenge is complicated by the fact that some patients may not even know they are infected. Care in the prehospital environment continues to focus on supporting the patient’s ventilation and circulation, while minimizing COVID-19 exposure to providers. In “Part 5: Public Health Implications,” the next excerpt from Evolution of EMS: COVID-19 Guidance for EMS Providers, we’ll discuss how changes in protocols and guidelines are helping to limit the spread of this disease.
References
American Thoracic Society. 2020. “Top 20 Pneumonia Facts—2019.” https://www.thoracic.org/
patients/patient-resources/resources/top-pneumonia-facts.pdf. Accessed October 13, 2020.
Burk, M, Karim El Kersh K, Saad M, Wiemken T, Ramirez J, Cavallazzi R: Viral infection in community-acquired pneumonia: A systematic review and meta-analysis. Eur Respir Rev 2016,25:178-88.
Calfee, CS, Delucchi K, Parsons PE, et al: Subphenotypes in acute respiratory distress syndrome: Latent class analysis of data from two randomised controlled trials. Lancet Respir Med 2014;2(8),611-620.
Caputo N, Strayer RJ, Levitan R: Early self-proning in awake, non-intubated patients in the emergency department: A single ED’s experience during the COVID-19 pandemic. Acad Emerg Med 2020;27(5):375-378.
Carpenter CR, Mudd PA, West CP, et al: Diagnosing COVID-19 in the emergency department: A scoping review of clinical examinations, laboratory tests, imaging accuracy, and biases. Acad Emerg Med 2020. June 16;10.1111/acem.14048.
Coppo A, Bellani G, Winterton D, et al: Feasibility and physiological effects of prone positioning in non-intubated patients with acute respiratory failure due to COVID-19 (PRON-COVID): A prospective cohort study. Lancet Respir Med 2020;8(8):765-774. https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(20) 30268-X/fulltext.
Cummings MJ, Baldwin MR, Abrams D, et al: Epidemiology, clinical course, and outcomes
of critically ill adults with COVID-19 in New York City: A prospective cohort study. Lancet 2020;395(10239):1763-1770.
Famous KR, Delucchi K, Ware LB, et al: Acute respiratory distress syndrome subphenotypes respond differently to randomized fluid management strategy. Am J Respir Crit Care Med 2017;195(3):331-338.
Fu Z, Tang N, Chen Y, Ma L: CT features of COVID-19 patients with two consecutive negative RT-PCR tests after treatment. Sci Rep 2020;10(1):11548.
Heneghan C, Pluddemann A, Mahtani KR: Differentiating viral from bacterial pneumonia. Centre for Evidence-Based Medicine website. https://www.cebm.net/covid-19 /differentiating-viral-from-bacterial-pneumonia/. Updated April 8, 2020. Accessed October 13, 2020.
Iba T, Levy JH, Levi M, Connors JM, Thachil J: Coagulopathy of coronavirus disease 2019.
Crit Care Med 2020; 48(9):1358-1364.
Infectious Diseases Education and Assessment. Convalescent plasma. https://covid.idea.
medicine.uw.edu /page/treatment/drugs/human-coronavirus-immune-plasma-hcip. Accessed October 13, 2020.
Pei G, Zhang Z, Peng J, et al: Renal involvement and early prognosis in patients with COVID-19 pneumonia. J Am Soc Nephrol 2020;31(6):1157-1165.
Rezaie S: The RECOVERY trial: Dexamethasone for COVID-19? REBELEM website. https:// rebelem.com/the-recovery-trial-dexamethasone-for-covid-19/. Updated June 23, 2020. Accessed October 13, 2020.
Roche JA, Roche R: A hypothesized role for dysregulated bradykinin signaling in COVID-19 respiratory complications. FASEB J 2020;34(6):7265-7269.
Salehi S, Abedi A, Balakrishnan S, Gholamresanezhad A: Coronavirus disease 2019 (COVID-19): A systematic review of imaging findings in 919 patients. AJR Am J Roentgenol 2020;215(1):87-93.
COVID-19 research briefing. University of Birmingham website. https://www.birmingham.ac.
uk/university/colleges/mds/Coronavirus/COVID-19-research-briefing.aspx. Accessed October 13, 2020.
US Department of Health and Human Services. Emergency use authorization declaration. Federal Register. https://www.federalregister .gov/documents/2020/04/01/2020-06905/emergency-use-authorization-declaration. Accessed October 13, 2020.
Coronavirus treatment acceleration program (CTAP). US Food and Drug Administration website. https://www.fda.gov/drugs /coronavirus-covid-19-drugs /coronavirus-treatment-acceleration-program-ctap. Updated September 30, 2020. Accessed October 13, 2020.
Ye Q, Wang B, Mao J: The pathogenesis and treatment of the ‘Cytokine Storm’ in COVID-19. J Infect 2020;80(6):607-613.