3d3bb467-e9ed-4611-87cd-e46c025ac32b.webp?sfvrsn=a1b7a841_3 "9781284229417-1-(1)")
 This is the first post in a five-part series where we'll give you a look inside this important new COVID-19 resource.
This is the first post in a five-part series where we'll give you a look inside this important new COVID-19 resource.
As an EMS provider, staying safe through the evolving COVID-19 situation involves distinct challenges. That's why the Public Safety Group, in partnership with the American Academy of Orthopaedic Surgeons, is pleased to introduce Evolution of EMS: COVID-19 Guidance for EMS Providers. This unique resource offers strategies and insights designed specifically for you.
In the excerpt below, we look at the SARS-CoV-2 virus itself, including a review of coronaviruses in general and the distinct challenges of diagnosing and treating this disease.
Evolution of EMS: COVID-19 Guidance for EMS Providers describes the SARS-CoV-2 virus and disease, prevention tactics, vaccine development, treatment, and public health implications, particularly as they affect providers working in the field. It’s not designed to supply everything you need to know about COVID-19, but rather to brief you on key issues and considerations. COVID-19 Guidance for EMS Providers also offers references for learning more and staying up to date. The goal: empowering you to protect yourself, your co-workers, and those you serve more efficiently and effectively.
There are three easy ways to access COVID-19 Guidance for EMS Providers:
- Stay Tuned to the Public Safety Group Blog:
New excerpts will be rolled out on our Public Safety Group blog on a biweekly basis, free of charge (Part One is available below, Part Two is available here, and Parts Three through Five will be available in the coming weeks)
- Sign Up to Receive a Free, Complete Copy of the Resource:
Visit http://go.psglearning.com/COVIDGuidanceNow to request your free copy today. We'll email you a PDF to download as soon as the complete resource is available later this Fall:
I Want to Request My Free PDF:
- Purchase Physical Copies of the Resource on our Website:
Visit http://go.psglearning.com/COVIDGuidance to pre-order your physical copy which will be available later this Fall
Questions? Please contact your dedicated Public Safety Specialist today.
Part One: Understanding COVID-19 Infection and Illness
Effective protocols and precautions for working with patients who have COVID-19 start with a basic understanding of severe acute respiratory syndrome coronavirus 2, or SARS-CoV-2, the virus that causes the COVID-19 disease.
Coronaviruses: An Overview
SARS-CoV-2 is a type of coronavirus. As such, it shares some important characteristics with other coronaviruses.
All viruses are microscopic in size, several times smaller than bacteria. They contain either RNA or DNA but cannot reproduce without a host. A virus spreads by invading host cells and then using the structure of the host’s cells to replicate. Thus, viruses have been referred to as intracellular parasites. Treatment of viral illnesses is tricky because viruses can gain access to the inside of the host’s cells and essentially hide. Viruses exist throughout nature and across all known species. Some viruses infect only nonhuman species, while others can infect both nonhumans and humans.
Coronaviruses contain RNA and belong to the virus family Coronaviridae, falling within one of two broad subcategories: Coronavirinae and Torovirinae. Both groups contain viruses found in nonhumans, but only those in the Coronavirinae group are known to cause disease in humans (Burrell 2017).
The name coronavirus comes from the Latin word corona, which means crown. It refers to the distinctive, crown-like appearance of the projections located on the protective envelope surrounding the virus’s genetic material (Figure 1-1). These projections are what enable the virus to attach to the host’s cells.
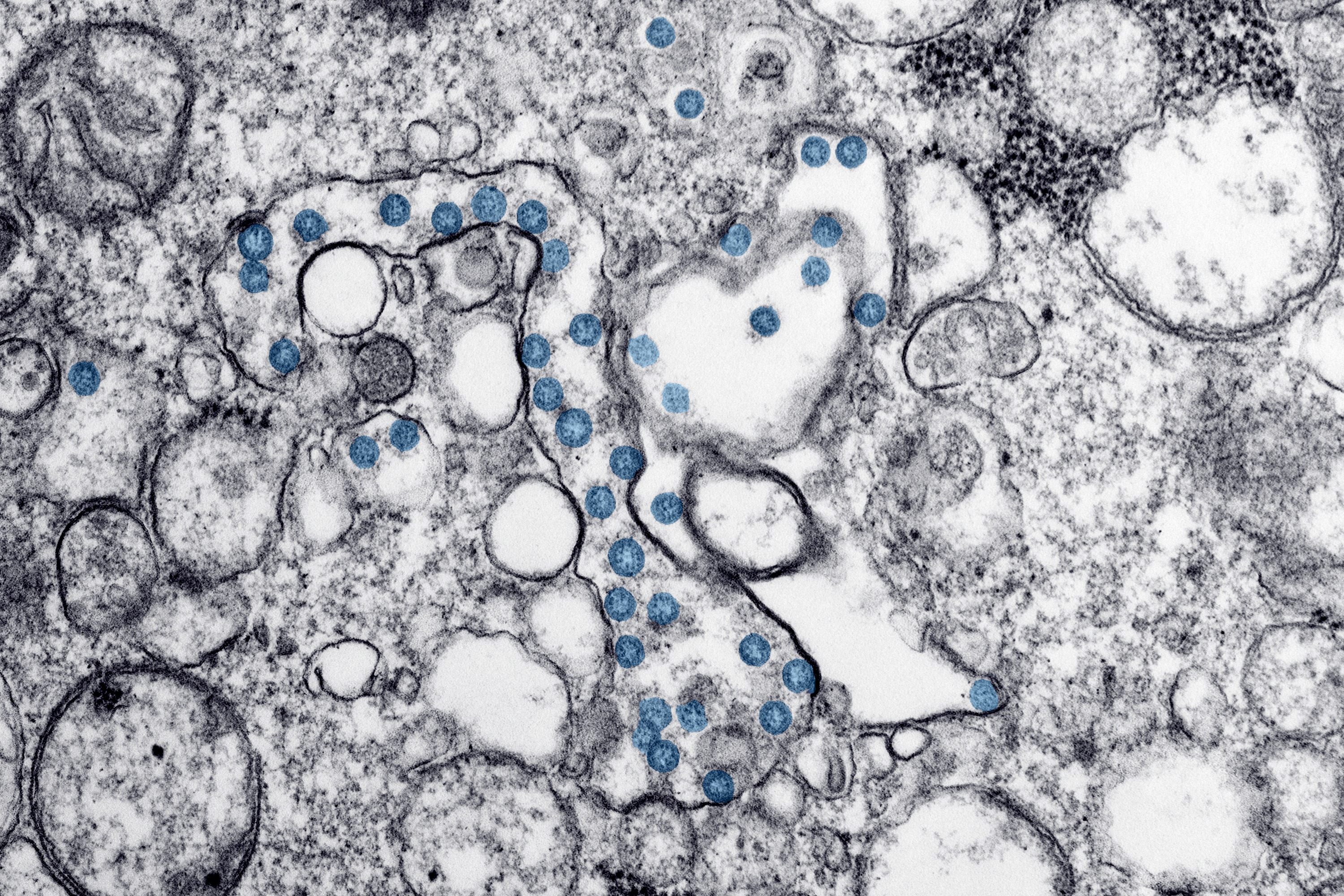 Figure 1-1: Ultrastructure of a coronavirus.
Figure 1-1: Ultrastructure of a coronavirus.
Courtesy of CDC/Alissa Eckert, MSMI; Dan Higgins, MAMS.
Where Coronaviruses Come From
Although the exact origin of coronaviruses is not known, the first incidence of this type of virus was identified in chickens in the 1930s. In the 1960s, a human coronavirus, distinct from more common rhinoviruses, was identified as a cause of the common cold in approximately 2% to 10% of patients experiencing cold-like symptoms (Korsman 2012).
Human coronaviruses were not considered a serious concern to humans until 2003, when a coronavirus responsible for causing severe acute respiratory syndrome (SARS) became evident. Originally found in nonhuman animals, including bats and civet cats (a species native to tropical Asia and Africa), the virus adapted and spread to humans. SARS affects the upper and lower respiratory systems and causes coughing, sneezing, runny nose, and pneumonia.
In 2003, approximately 8,000 probable SARS cases were reported to the World Health Organization (WHO), with 774 related deaths, a case fatality rate of 9.6%. WHO declared a pandemic, indicating the virus had spread rapidly throughout multiple countries. Governments responded with travel limitations and other precautions, and the spread of SARS was halted. Currently, there is no known human-to-human spread of SARS-CoV, but reemergence of the virus remains possible in the future from nonhuman reservoirs (Haagmans 2009).
Middle Eastern respiratory syndrome (MERS-CoV) is another example of a coronavirus. It first presented in 2012 in Saudi Arabia. Experts believe the virus originated in nonhuman hosts (camels) and transferred to humans. The virus transfers from human to human via respiratory secretions and is often spread from ill patients to those living with or caring for them. According to the Centers for Disease Control and Prevention (CDC), the MERS mortality rate is 30% to 40%. MERS-CoV is mostly confined to the Middle East and currently poses no large threat to those living in the United States.
Bats and other animals remain the primary infection reservoirs for coronaviruses. Most coronaviruses remain nonhuman-based, with just a few affecting humans (Table 1-1).
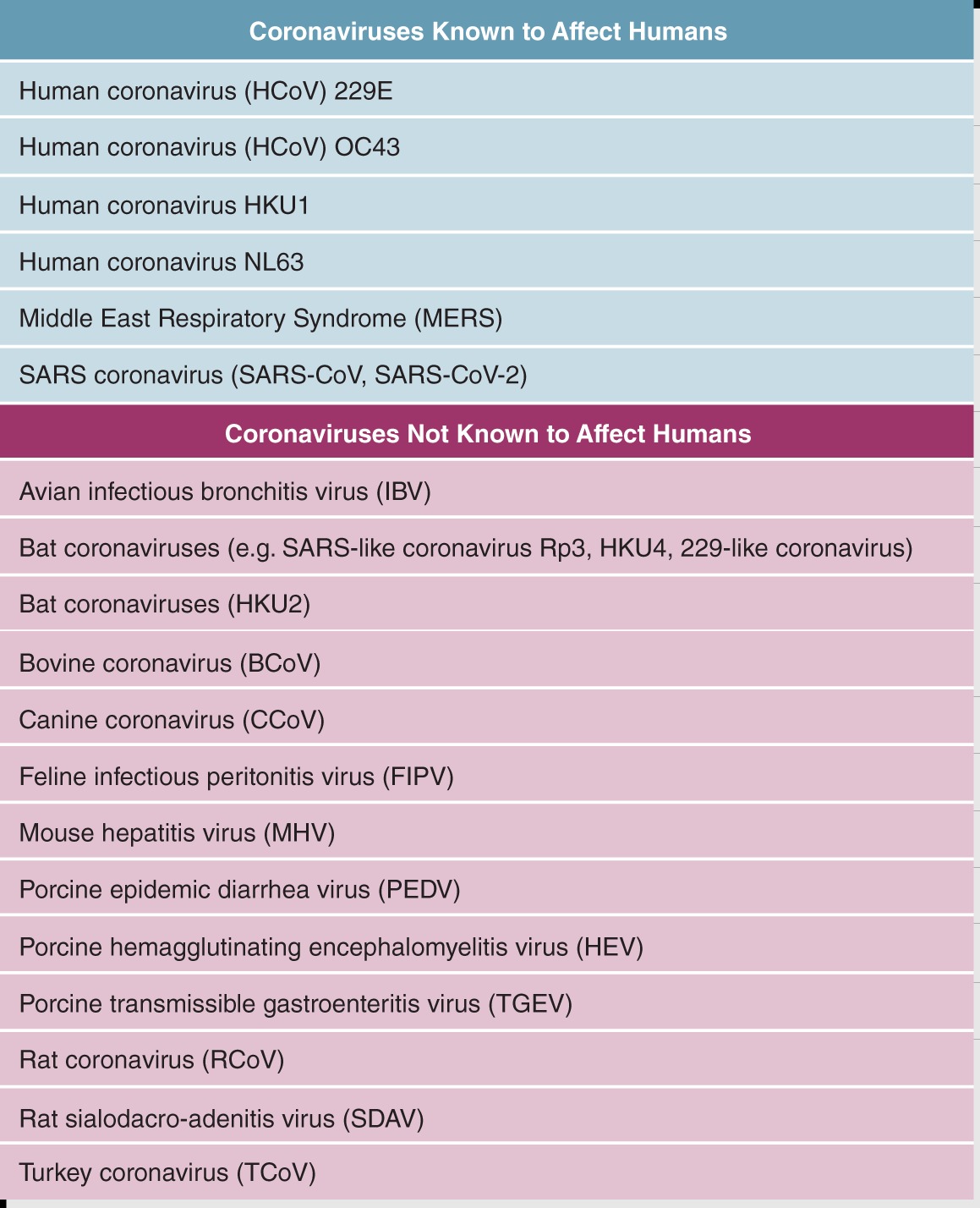 Table 1-1: Types of Coronaviruses
Table 1-1: Types of Coronaviruses
Adapted from Medical Microbiology, 18th Edition (Churchill Livingstone). Adapted from Centers for Disease Control and Prevention. 2020. “Human Coronavirus Types.” Accessed October 6, 2020.
When coronaviruses adapt and spread to humans, they can cause illness predominantly in the respiratory system. Patients commonly present with cold- and flu-like symptoms, including fever, cough, runny nose, and difficulty breathing. Older adults and people with preexisting medical conditions tend to become sicker than their younger, healthier counterparts. In patients with underlying medical conditions such as heart disease, diabetes, hypertension, and immune system compromise pneumonia may be more likely to develop and some even die from the virus.
How Coronaviruses Spread
Diseases that are transmitted between animals and humans are known as zoonotic. In some cases, coronaviruses can spread from nonhuman hosts to humans, but not from human to human unless the virus adapts. Viruses that do spread from human to human, such as MERS-CoV and SARS-CoV-2, commonly do so through respiratory droplets and aerosolized particles produced during coughing, sneezing, or talking.
It is also possible for people to become infected with coronavirus by touching a fomite, an object or surface contaminated with the virus, and then touching their eyes, nose, or mouth. Fomites can include door handles, tables, countertops, condiment dispensers, pens, and other items in public areas handled by multiple individuals. Fomite transmission is not considered the primary mode of transmission of COVID-19; however, contact with infectious surfaces still poses a risk of infection (Wilson, Corbett, and Tovey 2020).
Although surface contamination is not thought to be the primary mode of transmission, both symptomatic and asymptomatic patients can transmit the virus onto surfaces or to those with whom they come in contact. Once an individual is exposed to the virus, the incubation time—that is, the time it takes for symptoms to develop—can be 2 to 14 days.
COVID-19: A Closer Look
The SARS-CoV-2 virus, which causes COVID-19, is a novel virus, which means it is newly identified. Some of the earliest documented identifications of the virus occurred in December 2019, in the Hubei Province of China. Approximately 24 patients in one community presented with signs and symptoms of lung infection, quickly designated as a novel community-acquired pneumonia (CAP).
The name COVID-19 reveals much about the origin and nature of this disease: CO for corona, VI for virus, D for disease, and 19 for the year it was identified, 2019. The SARS-CoV-2 virus, as with other coronaviruses, was first identified in bats and other animals. When this virus adapted and spread to humans, it transmitted easily to other humans, resulting in a pandemic.
From Disease to Pandemic
With the rapid transmission of SARS-CoV-2, many people became ill in a short time. With communities not knowing exactly what the illness was or how to manage it, hospitals quickly filled up, creating a shortage of hospital beds—specifically, intensive care hospital beds. Medical facilities also experienced a shortage of necessary equipment, such as ventilators. Inadequate supplies of personal protective equipment (PPE) for health care workers meant many were asked to care for patients wearing the same face mask for several days, or until it was visibly soiled. This lack of appropriate PPE put providers at greater risk of becoming ill themselves.
EMS agencies had to evaluate their procedures, both to limit their providers’ exposure to the virus and to avoid the risk that providers would become vectors for COVID-19 transmission, spreading the virus as they moved from scene to scene throughout a community. Response protocols in many EMS systems changed dramatically. In March 2020, WHO declared COVID-19 a global pandemic, and countries across the world imposed guidelines to help limit the spread of the illness.
Mortality Rates
Initial estimates suggested that the mortality rate of COVID-19 might be as high as 7%, dramatically higher than that of other diseases such as influenza, which has a mortality rate of less than 1% (Table 1-2). As researchers continue to learn more about COVID-19, and as medical treatment for it has evolved through science and experience, the mortality rate for those infected has become much lower. By September 2020, the CDC calculated the COVID-19 mortality rate at slightly less than 5%. This figure is still in flux, as there is much discussion about the parameters used to calculate the infection and mortality rates.
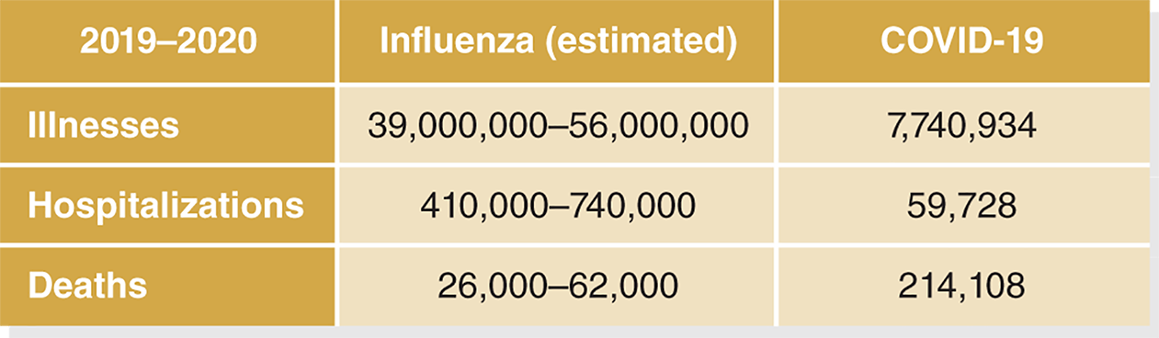
Table 1-2: Flu and COVID-19 Estimates
Data from Centers for Disease Control and Prevention. 2020. “2019–2020 US Flu Season: Preliminary In-Season Burden Estimates.” Accessed October 6, 2020.
“COVIDView Summary Ending October 3, 2020.” Accessed October 12, 2020.
The decrease in mortality rate reflects the growing understanding that many people who have COVID-19 have no symptoms or only minor symptoms. Thus, because the total number of people with COVID-19 is higher than the numbers initially reflected, the actual mortality rate is lower. Communities will determine morbidity and mortality rates as more data become available.
To better understand mortality rates and COVID-19, it is also important to consider excess mortality, a concept that refers to the rate of death during a crisis that is beyond what would be considered normal during that time.
Death rates during a set period of time can be predicted based on data from previous years. During a pandemic, overall death rates may increase, but the entirety of this increase does not necessarily represent people who died from the pandemic disease itself. In the case of COVID-19, the number of deaths during the pandemic has been higher than would have been expected without the pandemic.
Many of these deaths can be directly attributed to COVID-19 while others are only indirectly associated with COVID-19. For example, the stress on the healthcare system due to COVID-19 may have limited the ability of people with other conditions to receive care. In some instances, people elected not to seek medical care for medicalconditions because of concerns about being exposed to COVID-19. In other cases, the economic shutdown imposed to limit spread of the virus resulted in hardship that led to increased suicide rates, decreased ability to afford prescription medications, and other lifestyle changes that resulted in some level of increased mortality. Some deaths from unknown causes in certain communities may have been counted as unrelated to COVID-19 when, in fact they actually represented death from pandemic related viral illness.
For all of these reasons, understanding the true impact of the pandemic on mortality requires a more sophisticated approach than simply measuring Covid-19 confirmed deaths.
Testing and Diagnosis
COVID-19 is diagnosed by detection of the virus. One prevalent method involves collecting posterior nasal cavity cells with a swab. The swab is gently twisted in the nasopharyngeal cavity for several seconds to collect cells that are then examined for the presence of the virus’s RNA. Another method collects cells from an individual’s saliva instead. A negative test result suggests that the patient is not currently infected and cannot spread the illness. Some current guidelines allow an individual who tests negative to return to work or school immediately.
Once exposed to an illness, the human body develops antibodies to help prevent illness if exposed to the pathogen again. A blood test can identify the presence of SARS-CoV-2 antibodies, which indicates the patient has been previously exposed to SARS-CoV-2 and may have an immunity to it. This antibody testing provides additional data in determining incidence and prevalence of a disease in a population. However, currently it is not known how long a healthy individual with positive SARS-CoV-2 antibody results would be considered safe from reinfection or what antibody levels are necessary to confer functional immunity from reinfection. Some versions of the test require only a small finger stick to extract blood. The results of the test can be obtained in hours or days, depending on the laboratory or site where the test was conducted.
Although infection and antibody tests are crucial for understanding and controlling the spread of COVID-19, it is essential to recognize the limits of testing. The supply chain of testing products is improving, but some areas still experience delays in both receiving testing supplies and processing the tests. These delays have cascading effects; without test results, workers cannot return to the job, students cannot return to school, and contact tracing cannot be conducted to identify people who may have been exposed to individuals who test positive.
In addition, without comprehensive contact tracing, testing provides only a snapshot in time. A negative result today does not mean the person will be negative if tested again tomorrow, if the person has been interacting with others since the time of initial testing.
Also, not all tests are equally useful. In March 2020, the US Food and Drug Administration (FDA) issued a policy allowing developers of serologic tests to market them once the developer deemed them accurate. Since this policy was introduced, some firms have falsely claimed their tests are FDA-approved and have overstated their accuracy (FDA 2020).
It is also important to remember that a COVID-19 test can return false-positive results (incorrectly indicating that a particular condition or attribute is present) or false-negative results (incorrectly indicating that a particular condition or attribute is absent). A false-positive result can lead to a person being unnecessarily quarantined. Even more concerning, a false-negative result can lead infected patients to believe they can safely interact with others.
Given these variables, it is crucial to interpret COVID-19 test results carefully, following recommendations from the CDC and WHO (Figure 1-2).
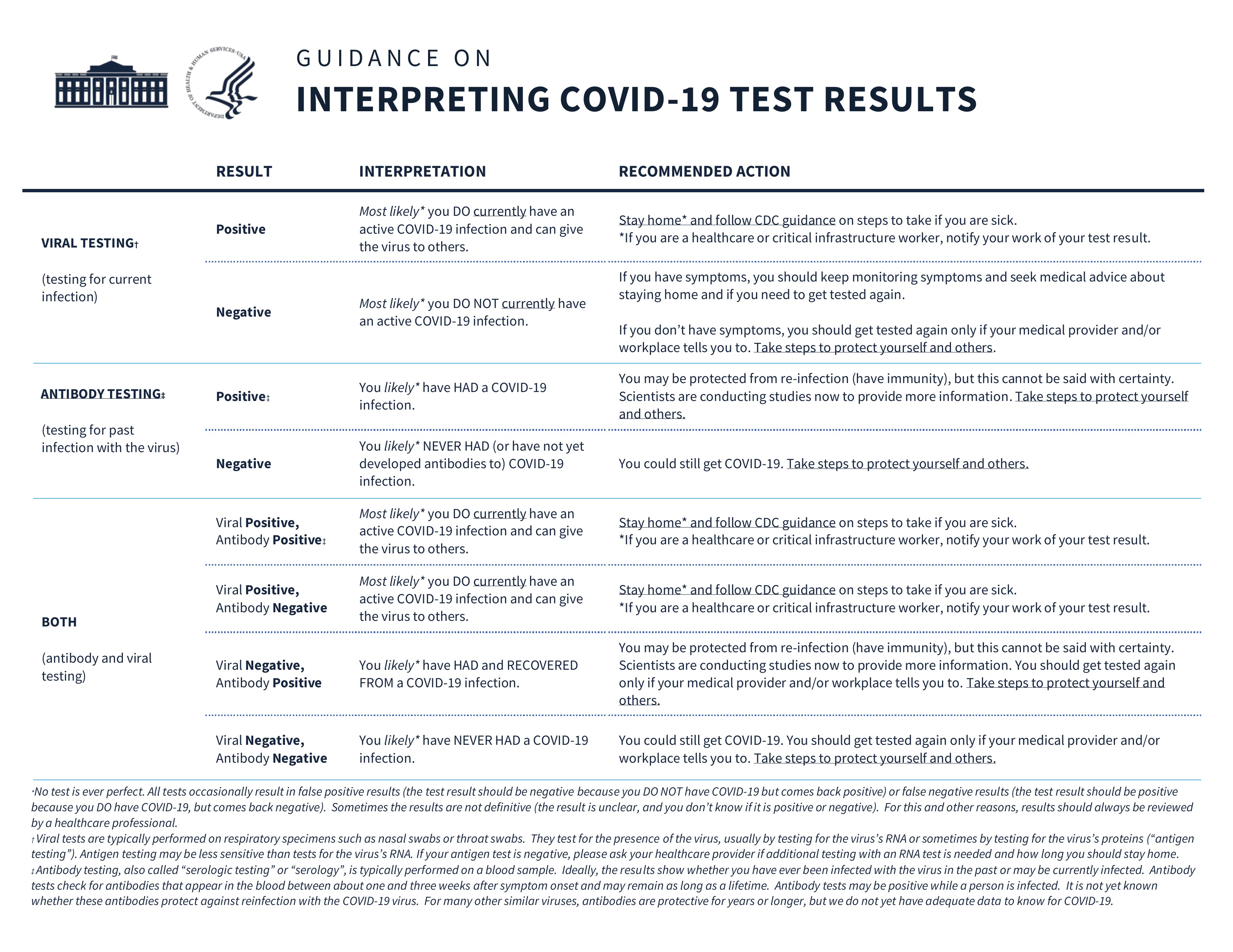
Figure 1-2: Guidance on interpreting COVID-19 test results
Reproduced from Department of Health and Human Services. 2020. “Guidance on Interpreting COVID-19 Test Results, The White House. Accessed October 6, 2020.
Scope of the Disease
When someone becomes infected with SARS-CoV-2, the virus attaches to the same cellular receptors as angiotensin-converting enzyme 2 (ACE-2). Cells with ACE-2 receptors are abundant in the lungs, although these cells also exist throughout the vasculature. Symptoms of COVID-19 may include cough, a loss of smell and/or taste, nausea and vomiting, diarrhea, congestion, sore throat, fatigue, and muscle or body aches.
It is important to note that some patients may not experience classic signs and symptoms, yet are still infected and capable of transmitting the virus to others. A concern with these carriers is the danger of asymptomatic spread. In the absence of symptoms, the infected person may continue to go to work and interact with others in public places, unknowingly exposing others to the virus and further spreading the disease.
Experts are still learning about the damage the SARs-CoV-2 virus is capable of causing. In most cases, as with the common cold caused by a coronavirus, the body’s immune system mounts an effective response to the virus and eradicates it, and the patient fully recovers. When healthy individuals become symptomatic with COVID-19, their symptoms typically last for up to 2 weeks. But even otherwise healthy patients can experience complications, including prolonged symptoms, an extreme overreactive immune response, and even death. In older adults and those with chronic medical conditions such as hypertension and diabetes, these side effects are more common.
Long-term effects of the disease are not yet fully understood and can involve neurologic, hematologic, and respiratory sequelae. Some severe cases progress to multiorgan failure or to acute respiratory distress syndrome (ARDS). With ARDS, the lung tissue becomes damaged, the alveoli in the lungs begin to fill with fluid, and the ability to transfer oxygen into the blood is hindered. Patients with ARDS can die secondary to hypoxia. It is possible for patients to die from sepsis because the infection overwhelms their body’s defenses (Figure 1-3).
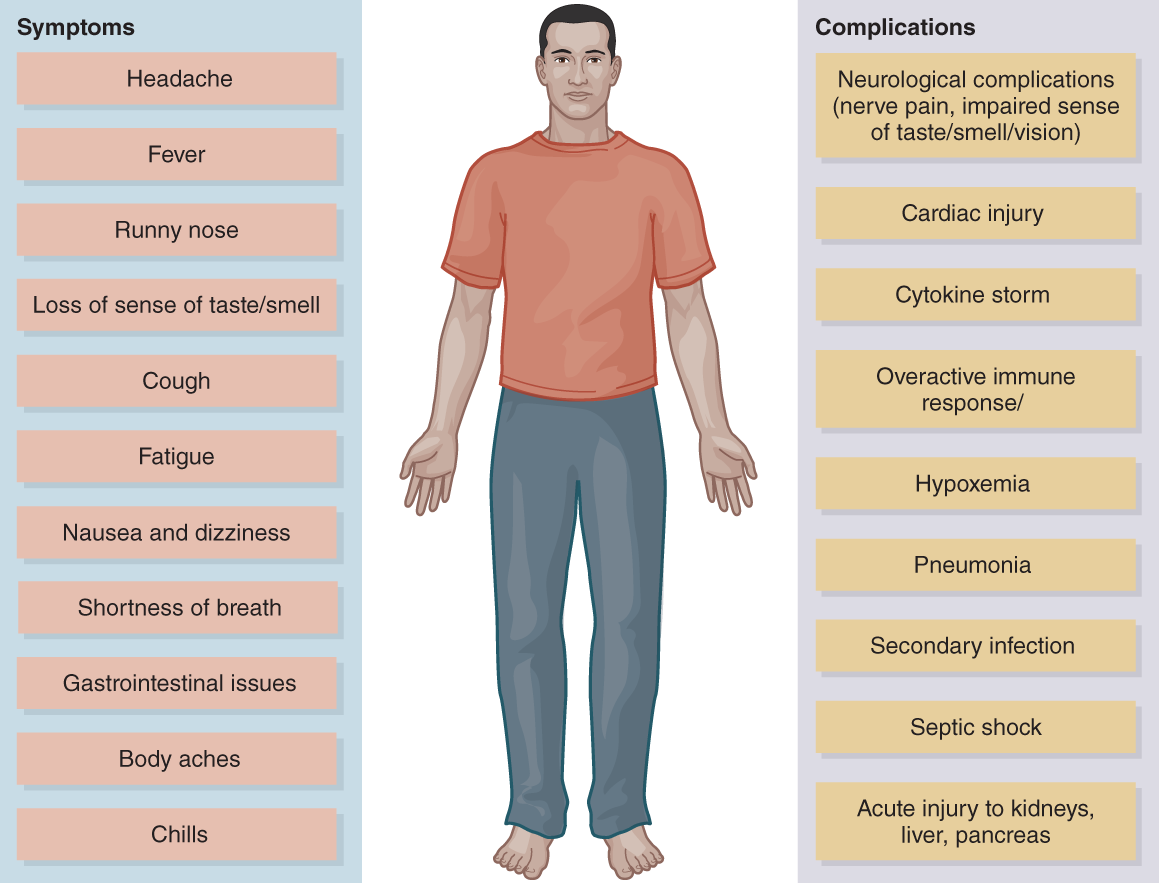 Figure 1-3: COVID-19 symptoms and complications
Figure 1-3: COVID-19 symptoms and complications
Jones & Bartlett Learning.
Most survivors of COVID-19 experience few or no lasting effects. For others, long-term complications can include scarring of the lung tissue (pulmonary fibrosis), which may cause respiratory problems later in life. In some survivors, coagulopathy (abnormal blood clotting), including disseminated intravascular coagulation (DIC), develops. With DIC, a person’s blood clots faster than normal. Clotting factors in the blood are rapidly depleted as a result, eventually leading to an inability to form further clots and then uncontrollable bleeding in some patients. In others, the clotting phase of the illness has been associated with an increased incidence of stroke and myocardial infarction secondary to the COVID-19 illness.
Much more needs to be learned about COVID-19, and research is ongoing. For instance, the disease was initially thought to be nonrelapsing, but a limited study of repeat cases suggests this may not always be true. Some patients in whom COVID-19 was diagnosed and were admitted to hospitals for treatment later experienced a recurrence of symptoms. During the relapses, the duration of symptoms was slightly shorter and younger, healthier patients required no hospitalization. Older patients with comorbidities required readmission (Gousseff, Penot, Gallay, et al. 2020).
The still-evolving body of authoritative knowledge about COVID-19 makes prevention strategies, including both nonpharmacologic interventions (eg, use of face masks and social distancing) and vaccines, crucial in controlling the spread of the virus.
Fortunately, prevention strategies, such as non-pharmacologic interventions, have shown great success in controlling the spread of the SARS-CoV-2 virus. We’ll take a closer look at these strategies in the next excerpt from Evolution of EMS: COVID-19 Guidance for EMS Providers, “Nonpharmacologic Prevention Strategies.”
References
Burrell, Christopher J. 2017. Fenner and White's Medical Virology, 5th ed. London: Academic Press.
Centers for Disease Control and Prevention. 2015. “Information About Middle East Respiratory Syndrome.” Accessed October 6, 2020.
Centers for Disease Control and Prevention. 2020. “2019–2020 US Flu Season: Preliminary In-Season Burden Estimates.” Accessed October 6, 2020.
Centers for Disease Control and Prevention. 2020. “Human Coronavirus Types.” Accessed October 6, 2020.
Gousseff, Marie, Pauline Penot, Laure Gallay, et al. 2020. “Clinical recurrences of COVID-19 symptoms after recovery: Viral relapse, reinfection or inflammatory rebound?” Journal of Infection. Accessed October 6, 2020.
Haagmans, Bart. 2009. Vaccines for Biodefense and Emerging and Neglected Diseases. London: Academic Press.
Korsman, Stephen N. J. 2012. Virology. London: Chirchhill Livingstone.
US Food and Drug Administration. 2020. “Coronavirus (COVID-19) Update: Serological Tests.” Accessed October 6, 2020.
Wilson, Nick, Corbett Stephen, and Tovey Euan. 2020. “Airborne Transmission of COVID-19.” BMJ 2020, 370, m3206; Accessed October 6, 2020.